Proximal (long head) biceps rupture
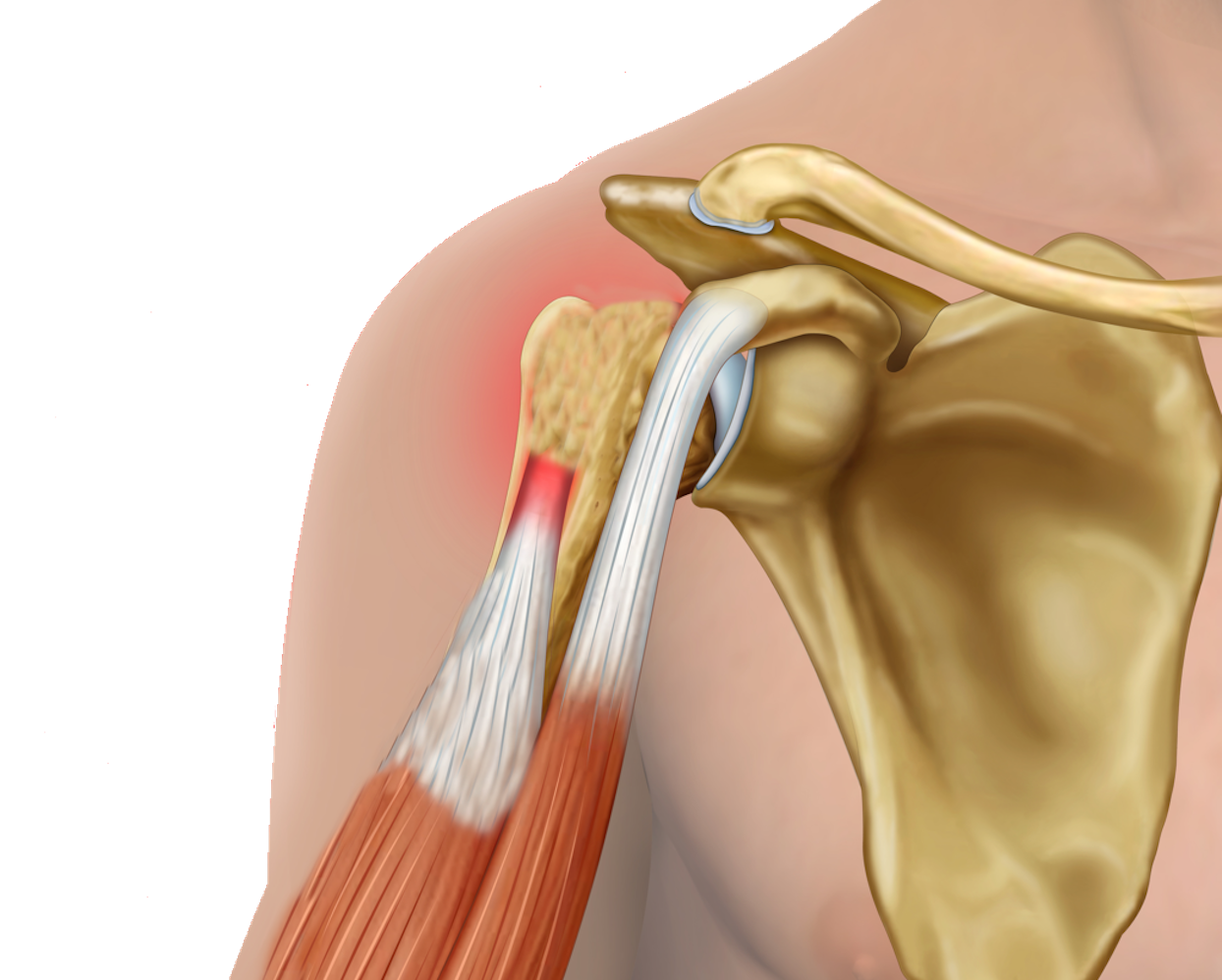
The biceps muscle is a muscle in the front of the upper arm. It has two attachments near the shoulder. The one at the front is where the short head of biceps attaches to the coracoid process (a boney prominence at the front of the shoulder). This is the important attachment for power in the arm. The other attachment of the biceps muscle is within the shoulder joint where the long head of biceps attaches to the glenoid. Because of the longer course that the long head of biceps (LHB) takes, it is at risk of irritation (tendinitis), or slipping out of its correct position which can cause pain and even damage the other tendons in the shoulder. If the long head of biceps has been irritated for a prolonged period it may fray like a worn rope and eventually rupture (snap).
While a long head of biceps tendon rupture doesn’t usually require any specific treatment, it can be associated with damage to other tendons in the shoulder so these are often assessed as they may require specific treatment or surgery.
In the context of a normal tendon, a rupture of the LHB is not usually an isolated injury and may indicate a more significant injury. Rupture in a degenerate tendon, where there has been gradual fraying and weakening of the tendon, can occur from a relatively minor event. Often there were preceding symptoms in the shoulder. In these cases, the LHB rupture is often an isolated event.
Often there is a long history of pain in the shoulder which is relieved when the LHB ruptures. With this event people often notice a bulge in their upper arm (‘popeye sign’), along with some cramping while the muscle settles into it’s new position.
There may be some initial weakness in the arm, but this usually improves and it is unusual to notice a significant functional weakness.
Avoiding exacerbating activities such as repeated overhead activities can help with the initial pain and cramping. In combination with this, simple painkillers are usually sufficient to control the discomfort associated with an LHB rupture while it settles.
It is very rare to need surgery for a spontaneous rupture of an LHB, however surgery may be required if there are associated tears or damage to other tendons in the shoulder.
This will depend on whether there are associated problems in the shoulder and can be discussed with your surgeon.
There is not usually a noticeable effect from an LHB rupture and even international sports people are able to play unaffected. The cosmetic deformity however will not change. This is different from a distal biceps tendon rupture which does lead to a small reduction in strength of flexion and supination and which are more commonly repaired.