Long head of biceps tendonitis
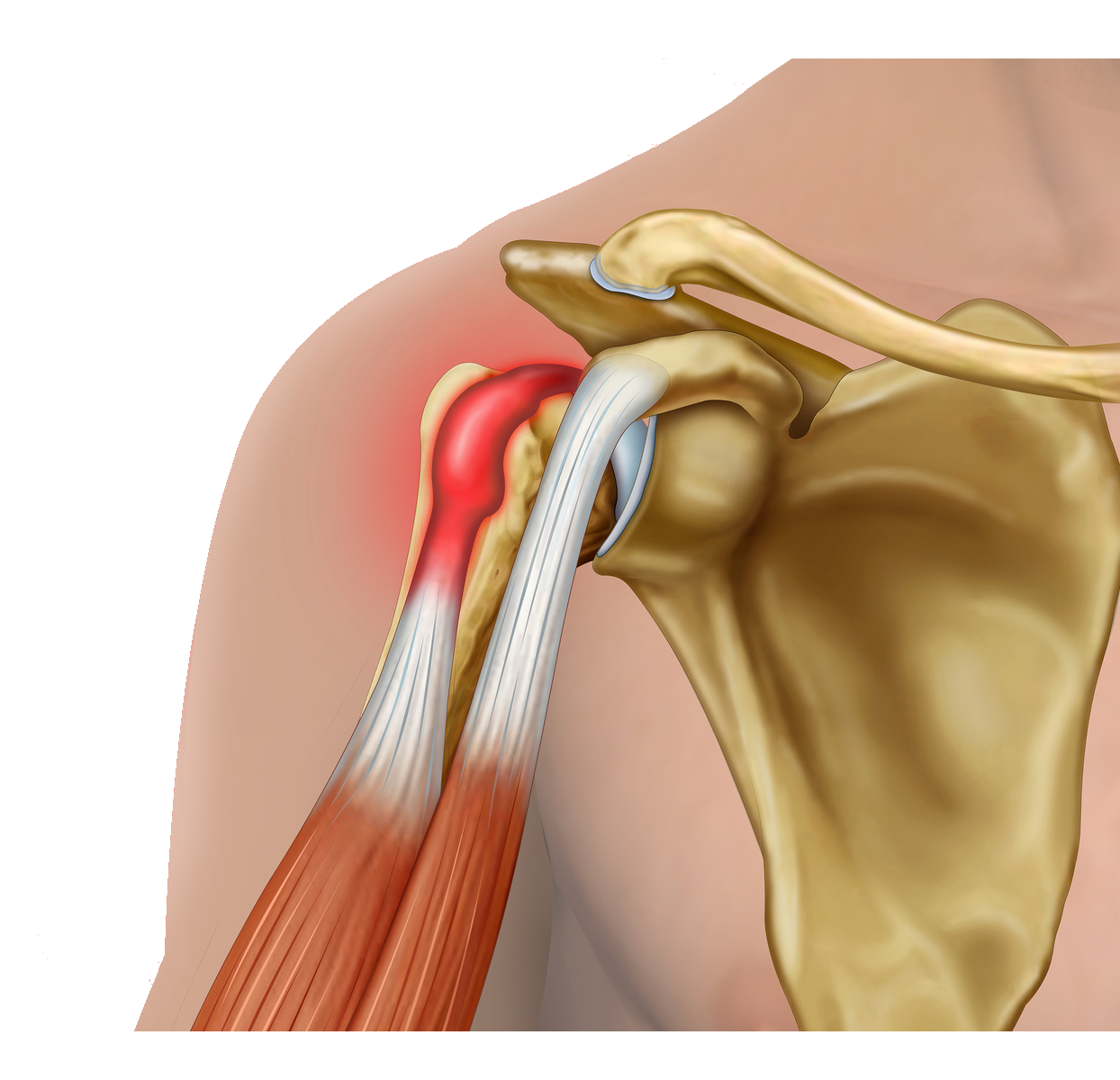
The biceps muscle is a muscle in the front of the upper arm. It has two attachments near the shoulder. The one at the front is where the short head of biceps attaches to the coracoid process (a boney prominence at the front of the shoulder). This is the important attachment for power in the arm. The other attachment of the biceps muscle is within the shoulder joint where the long head of biceps attaches to the glenoid. Because of the longer course that the long head of biceps (LHB) takes, it is at risk of irritation (tendinitis), or slipping out of its correct position which can cause pain and even damage the other tendons in the shoulder.
The LHB can fray if it slips out of its place which can happen if there is a tear in the front tendon of the shoulder. It can also cause pain if it becomes inflamed for any reason. While sometimes symptoms start after a specific injury or period of overuse, often there is no identified cause. More commonly the LHB frays and flattens over time with ageing.
Pain is the main symptom. There may also be tenderness at the front of the shoulder.
Usually simple painkillers and physiotherapy are sufficient to settle down the symptoms. Sometimes a steroid injection around the LHB tendon can help with the associated inflammation. In resistant cases, or where the biceps tendon has slipped out of it’s usual position, surgery may be advised.
In some cases the body releases the LHB tendon itself following a period of irritation and fraying, much like a rope frays and then breaks. In such cases a ‘pop’ may be felt followed by bruising and swelling around the shoulder. This often subsides and the previous irritation pain disappears and a bulge may be present in the upper arm, the ‘popeye sign’. There is no significant functional deficit associated with this.
The main surgical treatment is either to release the LHB (tenotomy) or to secure the tendon down away from it’s usual point of attachment (tenodesis). Which is best for you can be discussed with your surgeon. While either procedure can result in bunching of the biceps muscle (‘popeye’ sign), this is less frequent with a tenodesis. Sometimes if the tendon is secured (tenodesis) it may continue to cause discomfort from irritation further down the tendon path.
If a LHB tenotomy is performed as an isolated procedure, then you will have a sling for comfort for a few days, but can use your arm as comfort allows performing light two-handed activities at 2 weeks after surgery and moderate lifting at 6 weeks from surgery.
If only a LHB tenodesis is performed then you will have a sling for 3-4 weeks and commence light two-handed activities at 4-6 weeks and moderate lifting at 12 weeks.
People usually have good relief of symptoms after LHB surgery but it can take time for the muscle to accommodate to its new tension and people often experience initial cramping in the upper arm.